
Northwest Clinics, Alkmaar, the Netherlands
Dr. Mathijs Hendriks (Northwest Clinics)
Prof. dr. Sabine Siesling (IKNL/University of Twente)
Dr. Corina van den Hurk (Santeon hospitals)
Dr. Manon Hanrath-Komen (Northwest Clinics)
E: echemocoach@nwz.nl
Dr. Elise van Leeuwen-Stok (Clinical Study Manager BOOG)
Ilse Schilderinck, MSc (project assistant BOOG)
E: info@boogstudycenter.nl
Drs. Rubin Verduin (Northwest Clinics) (during maternity leave 21 June – 2 November temporary replaced by drs. Romi Sprengers)
E: echemocoach@nwz.nl
IKNL
IKNL
Dutch Cancer society (Dutch: KWF Kankerbestrijding)
The chosen research design for this study is a clinical prospective open-label 1:1 stratified randomized controlled intervention trial.
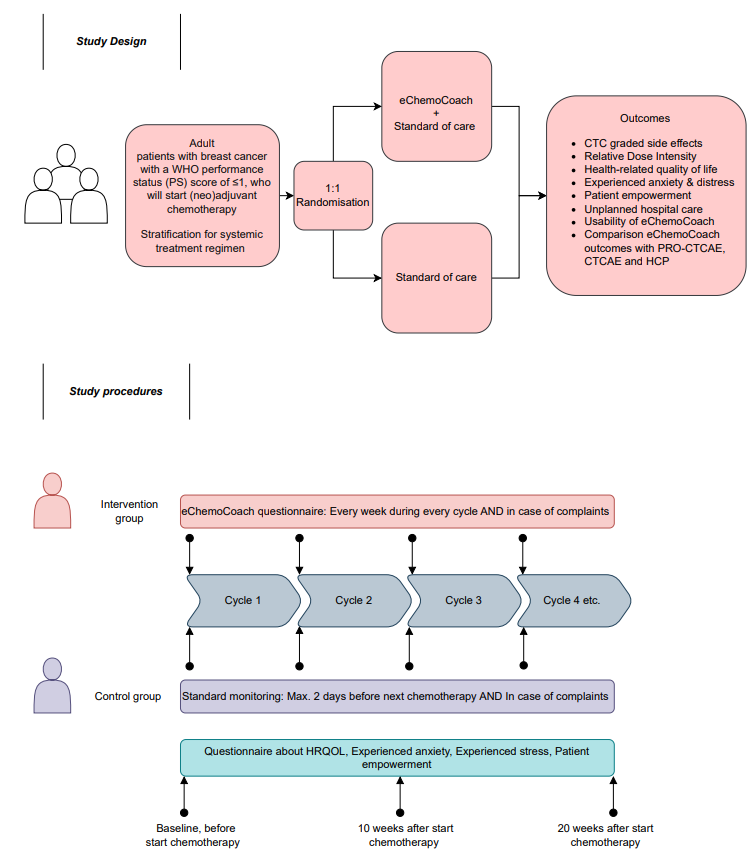
Primary objective:
To assess the effect of EHP-mediated monitoring and coaching via the eChemoCoach, in addition to usual care, on the occurrence of non-hematological side effects graded CTCAE ≥3 in breast cancer patients receiving neo-adjuvant or adjuvant chemotherapy.
Secondary objectives:
To determine the effect of applying EHP-mediated monitoring and coaching of patient reported side effects compared to standard of care on:
Further secondary objectives:
Primary endpoint:
The occurrence of non-hematological grade ≥3 side effects, as defined by the CTCAE version 5.0 criteria (see appendix A) during (neo) adjuvant chemotherapy in breast cancer patients.
Secondary endpoints:
To study the effect of EHP-mediated monitoring and coaching with the eChemoCoach on
Further endpoints:
Inclusion criteria:
Exclusion criteria: